




SKIN ULCERS: ULTRASOUND THERAPY AND COLLAGEN REGENERATION THERAPY
Innovative treatment of chronic skin ulcers of the lower limbs with ultrasonic treatment and a collagen membrane derived from heterologous pericardium and peritoneum
Edited by Antonio La Rosa M.D.
Professor of Surgery
Dep. of Vascular and Endovascular Surgery
University of Pavia, Italy
+ 39 339/7994760
+ 39 0382/24179
Ultrasounds have demonstrated to be highly effective in significantly reducing the healing time of skin ulcers of the lower limbs allowing to obtain in a very short time, even in a single sitting, the optimal wound cleansing associated with severe reduction of bacterial load
( GENERA ULTRASONIC - by Italia Medica srl ) (see SKIN ULCERS : ULTRASONIC TREATMENT). The ultrasound removal of deposits often tenaciously adherent to the bottom of the ulcer, allows for its optimal state of preparedness in accepting every therapeutic aids, such as advanced wound dressings, dermo epidermal graft, so that they can act without interference from necrotic, fibrotic, exudative materials and promote rapid healing. If the repair processes are particularly slow as in chronic skin ulcers, which show no signs of healing and remain unaltered for many months or years, it is essential to reignite the healing mechanism that, by personal experience, involves an innovative method of tissue regeneration with the use of ultrasound and collagen membrane derived from heterologous pericardium and peritoneum.
Reparative stages of skin ulcers and collagen
Through three reparative stages, defined respectively as the inflammation, proliferative and remodeling phase in cases of skin ulcer all biochemical processes and tissues are destined to the formation of the fundamental constituent of the tissues, collagen. The latter is the main protein of connective tissue, tissue scaffold in humans and in animals, acting as a link, support and nourishment of tissues of various organs and which forms the extracellular matrix (ECM). The initial formation of collagen is due to the migration of fibroblasts, cells from the subcutaneous tissue, triggered by the state of irritation or inflammation in the bottom skin ulcer. The production of collagen by fibroblasts induces the triggering of the proliferative phase with formation of granulation tissue i.e. reparative tissue of cutaneous ulcer whose task is to fill the large area of loss of substance. The product is primarily collagen type III, typical of the granulation tissue, which will require large amounts for the progress of the granulation process and therefore of growth of the tissue in the ulcer skin; the collagen type III is then gradually replaced by collagen type I, collagen which represents the definitive collagen and which represents 90% of the total collagen of the connective tissue of the skin.
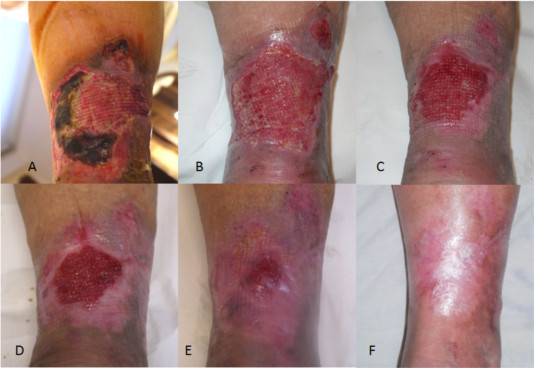
Case 1 - A: Chronic skin ulcer of mixed type, arterio-venous lower third of the leg, dating back over 5 years ( GENERA ULTRASONIC )(after ultrasound cleansing ), B: Application of collagen membrane, C: Result after 1 month of treatment with collagen membrane: the granulation tissue has filled the loss of substance of the skin ulcer, D: 3 months Result: reduction of the ulcer with the appearance of areas of epithelialization, E: Result at 3 and a half months of treatment with collagen membrane : progress of epithelialization of skin ulcer, F: Result at 4 months; G: Advanced skin ulcer resolution to 5 ½ months of treatment with collagen membrane, H: Complete resolution of skin ulcer at 6 months of treatment with collagen membrane
Slowing down of reparative stages of skin ulcers
This physiological process of collagen synthesis in the skin ulcer can slow down or stop the onset of a chronic lesion characterized by an arrest of the healing process in a stabilized inflammatory condition. The chronic skin ulcer that is to occur is therefore the expression of the presence of a high number of neutrophils and macrophages, immune cells that produce high amounts of inflammatory mediators. The latter stimulate the endothelial cells to produce exudates and proteolytic enzymes that cause tissue degradation and inhibition to the formation of a functional extracellular matrix (ECM) and then of collagen.
Therapeutic Prerogatives
The healing process of skin ulcers of the lower limbs, in order to start and move quickly toward recovery, require that the therapeutic procedure essentially fulfils three prerogatives:

Case 2 - V. L., age 77. Infected skin ulcer by staphylococcus aureus in the upper calcaneus region foot SX mixed (PAD + chronic venous insufficiency) with exposure of the Achilles tendon dating back about 5 months. A: ulcer prior to ultrasonic treatment. B: After cleansing and killing bacteria with ultrasound ( GENERA ULTRASONIC ). C: application of collagen membrane. D: on the 35th day of collagen treatment: reduction in ulcer size with partial coverage of the Achilles tendon. E: an advanced stage of resolution and re-epithelialization at the 68th day with total coverage of the Achilles tendon. F: complete resolution on the 97th day.
Removal of the primary causes of chronicization
Regarding the removal of the primary causes at the base of skin ulcer it is important to note that about 90% of skin ulcers of the lower extremities are of vascular origin (70-80% venous, arterial 10-15%, 3-5% mixed: arteriovenous and veno-venous-lymphatic), while in the remainder the following causes are recognized: trauma, haematological diseases, autoimmune diseases, metabolic, infectious and degenerative diseases. Often the prolonged healing time (sometimes years) is attributable to a non-effective treatment of the pathology underlying the onset of cutaneous ulcer in which case it is possible to observe either stationarity of the situation or in the worst cases a deterioration with increase in size of the lesion.
The favourable evolution towards healing can then, after removal or containment of the causes, develop through complex reparative stages leading at first to the reconstruction of the dermal tissue and finally to its epithelialization, with final closure of the ulcer skin.
It's still possible to observe that often the mere removal of the primary causes may not be sufficient for the healing of skin and you can watch a chronic lesion characterized by an arrest of the healing process in a stabilized inflammatory condition . The occurrence of chronic skin ulcer may occur due to the overlapping of adverse events such as infection of skin ulcer, chemical injury of ulcerative base (intolerance to topical drugs or medication), mechanical damage (too traumatic surgical curettage), immune cutaneous anergy associated diseases such as diabetes, anaemia, disvitaminosis and others to be identified in each case. The removal of the causes of chronicization must also be taken into account for the therapeutic treatment of the salient features of chronic skin ulcers: bacterial colonization, chronic inflammation, high levels of proteases, degradation of the ECM, the predominance of senescent fibroblasts, degraded or inactive growth factors.
Collagen treatment of chronic skin ulcers of the lower limbs
Rationale
The exogenous and therefore therapeutic application of collagen directly to the chronic skin ulcer presents itself as an ideal response to the treatment of slow-healing skin ulcers, characterized by a reduced reparative response in both stages of granulation and of reepithelialization, providing the substrate for the connective and epithelial regeneration.

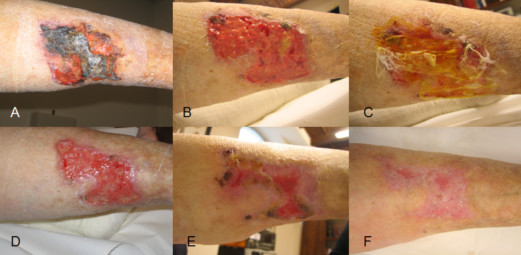
Case 3 - D. G. age 81 A: skin ulcer against the rear face of the right leg secondary to necrotizing capillaritis dating back 3 months. B: After ultrasonic treatment ( GENERA ULTRASONIC ). C: Application of segments of collagen membrane. D: On the 75th day of collagen treatment. E: Significant reduction in extent of the lesion to 105°F day of collagen therapy: complete resolution at the 187th day of collagen therapy.
Action Materials and mechanisms
By personal experience the collagen materials employed are represented by membranes derived from pig pericardium and peritoneum, consisting of collagen type I and III in the form of thin dried sterile membranes 300 - 400 micrometres or less thin, up to 0.5 mm (Tecnoss - TORINO). In order not to counteract the therapeutic efficacy of the membranes it is essential that the ulcerative base is subjected to radical debridement-cleansing, preferably ultrasonic ( GENERA ULTRASONIC - by Italia Medica srl ), for their high effectiveness in the removal of fibrin and their high bactericidal effect. With ulcerative base well cleansed and aseptic thanks to ultrasound, the membrane lying in it, after appropriate hydration, starts to perform its chemotactic action i.e. trigger for macrophages and fibroblasts which start to migrate from the periphery of the ulcer of skin to the ulcerative base.
The beginning of the healing process of granulation
Thus begins the process of granulation or cell replication. The macrophages through the production of growth factors stimulate cell replication and begin to digest the implanted collagen membrane that acts as a support and model to the new collagen produced by fibroblasts arrived on site, the latter also have the property to secrete hyaluronic acid which is essential for the formation of collagen fibers.
The porcine-derived collagen membrane as well as supporting the initiation of the granulation process by calling macrofagi and fibroblasts also serves as the inducer gene to direct fibroblast cell replication in the context of skin ulcer. Repeated application of the collagen membranes, in 8-10 days intervals, allows for the preservation of conditions that facilitate cell replication in cutaneous ulcer with reconstruction of the dermal tissue up to the total filling up of the skin ulcer to the epidermal limit. Once the connective tissue regeneration phase is completed the definitive dermal ulcer healing requires that the stage of epithelial regeneration is initiated.
Case 4 - I. G. age 80 A: Chronic skin ulcer extended to the right side of right leg dating back 1 year secondary to chronic venous and lymphatic insufficiency means loss of substance and ulcerative base about 3 mm from the skin surface. B: After 1 month of treatment with collagen therapy: reduction of the depth of the skin ulcer with ulcerative base at about 1 mm from the skin surface. C: To 3.5 months of treatment with collagen is completely filled up to the skin limit of the ulcerative base. D: Application of the collagen membrane to the periphery of the skin ulcer in order to promote epithelialisation. E - F: Removing collagen membrane previously applied through neo-epithelium below. G: Significant reduction in the extent of the lesion at 6 months of collagen therapy. H: 6.5 months. I: Complete healing 8 months after initiation of therapy.
Re-epithelialization of skin ulcers
The re-epithelialisation of skin ulcers, whether they are of recent onset or evolved in chronic skin ulcers, requires that a process of slipping and replication of epithelial cells free from trauma from is implemented the periphery towards the center. Repeated application and at 10-15 days intervals of collagen membrane placed at the outer edges of the skin ulcer enabled, in our experience, an effective and rapid re-epithelialization with a resolution of even large leg ulcers. The personal experience relates to the use of collagen membranes of varying thickness and, when aimed at initiation and preservation of the granulation process, chosen according to the extent of the loss of substance of cutaneous ulcer. The membrane in this case is totally reabsorbed from the ulcerative base and will no longer be found at the next dressing. In the phase of reepithelialization the collagen membrane used has a minimum thickness (300-400 micrometres) and acts as a protection to the sliding epithelial skin from the edges of the ulcer, will be found at the next dressing and adherent to the neo-epithelium (see description case 4) from which will be gradually removed.
Clinical Results
The clinical results with use of ultrasonic ( GENERA ULTRASONIC )treatment associated with collagen therapy in the treatment of skin ulcers of the lower extremities are by personal experience, very positive and innovative compared to conventional treatments. In particular, in addition to the benefits described above regarding the use of ultrasound related to debridement-wound cleansing and a significant reduction of the bacterial load (see article SKIN ULCERS: ULTRASONIC TREATMENT) the following has been observed:

Case 5 - S. N., age 79. Skin ulcer chronic lower limb DX dating back about 5 years, the region above the medial malleolus, in patient with lower extremity PAD (bearer of femoral popliteal bypass DX) and chronic venous insufficiency from previous DVT leg DX. A: After ultrasonic treatment. B: After application of collagen membrane segments. C: 20 days after initiation of collagen therapy. Q: 52 Day E: 72 °. F day: Full healing at 134th day with collagen therapy.

Case 6 - B. Ca91 post traumatic infected ulcerative lesion in the lateral malleolar right foot dating back over 13 months. A: After ultrasonic treatment ( GENERA ULTRASONIC ) and application of collagen membrane. B: After 17 days of treatment. C: Significant reduction of ulcerative region at day 30. D: At day 42. E: Complete resolution at day 65 of treatment with collagen membrane. F: Check-up 1 month after healing of cutaneous ulcer.
EQUIPMENT:
GENERA ULTRASONIC - by Italia Medica srl - info@italiamedicasrl.com - info@italiamedicaint.com
-------------
Bibliography
1) Ultrasonic Treatment of Infected Leg Ulcers: Results Preliminary. La Rosa A. et al. 15th World Congress of Phlebology of the Union Internationale de Phlebologie - Rio de Janeiro, October 2-7, 2005 ( GENERA ULTRASONIC - by Italia Medica srl Congress ).
2) Equine Pericardium Collagen Wound Dressing in the Treatment of the Neuropathic Diabetic Foot Wound. A Pilot Study. John G. Fleischli, DPM, Terese J. Laughlin, DPM and Jeffery W. Fleischli, DPM. Journal of the American Podiatric Medical Association. Volume 99 Number 4301-305 2009
3) Knapp TR, Kaplan EN, Daniels JR. Injectable collagen for soft tissue augmentation. Plast Reconstr Surg.1977; 60:398-405.
4) Knapp TR, Luck E, Daniels JR.Behavior of solubilized collagen as a bioimplant. J Surg Res 1977; 23:96-105.
5) Greenstein G, Caton JG. Biodegradable barriers and guided tissue regeneration. Periodontol 2000. 1993; 1:36-45.
6) Schlegel AK, Mohler H, F Busch, et al. Preclinical and clinical studies of a collagen membrane (Bio-Gide). Biomaterials. 1997; 18:535-538.
Edited by Antonio La Rosa M.D.
Professor of Surgery
Dep. of Vascular and Endovascular Surgery
University of Pavia, Italy
+ 39 339/7994760
+ 39 0382/24179
Ultrasounds have demonstrated to be highly effective in significantly reducing the healing time of skin ulcers of the lower limbs allowing to obtain in a very short time, even in a single sitting, the optimal wound cleansing associated with severe reduction of bacterial load
( GENERA ULTRASONIC - by Italia Medica srl ) (see SKIN ULCERS : ULTRASONIC TREATMENT). The ultrasound removal of deposits often tenaciously adherent to the bottom of the ulcer, allows for its optimal state of preparedness in accepting every therapeutic aids, such as advanced wound dressings, dermo epidermal graft, so that they can act without interference from necrotic, fibrotic, exudative materials and promote rapid healing. If the repair processes are particularly slow as in chronic skin ulcers, which show no signs of healing and remain unaltered for many months or years, it is essential to reignite the healing mechanism that, by personal experience, involves an innovative method of tissue regeneration with the use of ultrasound and collagen membrane derived from heterologous pericardium and peritoneum.
Reparative stages of skin ulcers and collagen
Through three reparative stages, defined respectively as the inflammation, proliferative and remodeling phase in cases of skin ulcer all biochemical processes and tissues are destined to the formation of the fundamental constituent of the tissues, collagen. The latter is the main protein of connective tissue, tissue scaffold in humans and in animals, acting as a link, support and nourishment of tissues of various organs and which forms the extracellular matrix (ECM). The initial formation of collagen is due to the migration of fibroblasts, cells from the subcutaneous tissue, triggered by the state of irritation or inflammation in the bottom skin ulcer. The production of collagen by fibroblasts induces the triggering of the proliferative phase with formation of granulation tissue i.e. reparative tissue of cutaneous ulcer whose task is to fill the large area of loss of substance. The product is primarily collagen type III, typical of the granulation tissue, which will require large amounts for the progress of the granulation process and therefore of growth of the tissue in the ulcer skin; the collagen type III is then gradually replaced by collagen type I, collagen which represents the definitive collagen and which represents 90% of the total collagen of the connective tissue of the skin.
Case 1 - A: Chronic skin ulcer of mixed type, arterio-venous lower third of the leg, dating back over 5 years ( GENERA ULTRASONIC )(after ultrasound cleansing ), B: Application of collagen membrane, C: Result after 1 month of treatment with collagen membrane: the granulation tissue has filled the loss of substance of the skin ulcer, D: 3 months Result: reduction of the ulcer with the appearance of areas of epithelialization, E: Result at 3 and a half months of treatment with collagen membrane : progress of epithelialization of skin ulcer, F: Result at 4 months; G: Advanced skin ulcer resolution to 5 ½ months of treatment with collagen membrane, H: Complete resolution of skin ulcer at 6 months of treatment with collagen membrane
Slowing down of reparative stages of skin ulcers
This physiological process of collagen synthesis in the skin ulcer can slow down or stop the onset of a chronic lesion characterized by an arrest of the healing process in a stabilized inflammatory condition. The chronic skin ulcer that is to occur is therefore the expression of the presence of a high number of neutrophils and macrophages, immune cells that produce high amounts of inflammatory mediators. The latter stimulate the endothelial cells to produce exudates and proteolytic enzymes that cause tissue degradation and inhibition to the formation of a functional extracellular matrix (ECM) and then of collagen.
Therapeutic Prerogatives
The healing process of skin ulcers of the lower limbs, in order to start and move quickly toward recovery, require that the therapeutic procedure essentially fulfils three prerogatives:
- removal or otherwise marked containment of the primary causes that led to the emergence of skin ulcer
- removal of the causes which have contributed to its eventual chronicization
- therapeutic use of aids that facilitate, strengthen and in some cases complement the reparative stages that once the causes are removed physiologically lead to healing of the skin.
Case 2 - V. L., age 77. Infected skin ulcer by staphylococcus aureus in the upper calcaneus region foot SX mixed (PAD + chronic venous insufficiency) with exposure of the Achilles tendon dating back about 5 months. A: ulcer prior to ultrasonic treatment. B: After cleansing and killing bacteria with ultrasound ( GENERA ULTRASONIC ). C: application of collagen membrane. D: on the 35th day of collagen treatment: reduction in ulcer size with partial coverage of the Achilles tendon. E: an advanced stage of resolution and re-epithelialization at the 68th day with total coverage of the Achilles tendon. F: complete resolution on the 97th day.
Removal of the primary causes of chronicization
Regarding the removal of the primary causes at the base of skin ulcer it is important to note that about 90% of skin ulcers of the lower extremities are of vascular origin (70-80% venous, arterial 10-15%, 3-5% mixed: arteriovenous and veno-venous-lymphatic), while in the remainder the following causes are recognized: trauma, haematological diseases, autoimmune diseases, metabolic, infectious and degenerative diseases. Often the prolonged healing time (sometimes years) is attributable to a non-effective treatment of the pathology underlying the onset of cutaneous ulcer in which case it is possible to observe either stationarity of the situation or in the worst cases a deterioration with increase in size of the lesion.
The favourable evolution towards healing can then, after removal or containment of the causes, develop through complex reparative stages leading at first to the reconstruction of the dermal tissue and finally to its epithelialization, with final closure of the ulcer skin.
It's still possible to observe that often the mere removal of the primary causes may not be sufficient for the healing of skin and you can watch a chronic lesion characterized by an arrest of the healing process in a stabilized inflammatory condition . The occurrence of chronic skin ulcer may occur due to the overlapping of adverse events such as infection of skin ulcer, chemical injury of ulcerative base (intolerance to topical drugs or medication), mechanical damage (too traumatic surgical curettage), immune cutaneous anergy associated diseases such as diabetes, anaemia, disvitaminosis and others to be identified in each case. The removal of the causes of chronicization must also be taken into account for the therapeutic treatment of the salient features of chronic skin ulcers: bacterial colonization, chronic inflammation, high levels of proteases, degradation of the ECM, the predominance of senescent fibroblasts, degraded or inactive growth factors.
Collagen treatment of chronic skin ulcers of the lower limbs
Rationale
The exogenous and therefore therapeutic application of collagen directly to the chronic skin ulcer presents itself as an ideal response to the treatment of slow-healing skin ulcers, characterized by a reduced reparative response in both stages of granulation and of reepithelialization, providing the substrate for the connective and epithelial regeneration.
Case 3 - D. G. age 81 A: skin ulcer against the rear face of the right leg secondary to necrotizing capillaritis dating back 3 months. B: After ultrasonic treatment ( GENERA ULTRASONIC ). C: Application of segments of collagen membrane. D: On the 75th day of collagen treatment. E: Significant reduction in extent of the lesion to 105°F day of collagen therapy: complete resolution at the 187th day of collagen therapy.
Action Materials and mechanisms
By personal experience the collagen materials employed are represented by membranes derived from pig pericardium and peritoneum, consisting of collagen type I and III in the form of thin dried sterile membranes 300 - 400 micrometres or less thin, up to 0.5 mm (Tecnoss - TORINO). In order not to counteract the therapeutic efficacy of the membranes it is essential that the ulcerative base is subjected to radical debridement-cleansing, preferably ultrasonic ( GENERA ULTRASONIC - by Italia Medica srl ), for their high effectiveness in the removal of fibrin and their high bactericidal effect. With ulcerative base well cleansed and aseptic thanks to ultrasound, the membrane lying in it, after appropriate hydration, starts to perform its chemotactic action i.e. trigger for macrophages and fibroblasts which start to migrate from the periphery of the ulcer of skin to the ulcerative base.
The beginning of the healing process of granulation
Thus begins the process of granulation or cell replication. The macrophages through the production of growth factors stimulate cell replication and begin to digest the implanted collagen membrane that acts as a support and model to the new collagen produced by fibroblasts arrived on site, the latter also have the property to secrete hyaluronic acid which is essential for the formation of collagen fibers.
The porcine-derived collagen membrane as well as supporting the initiation of the granulation process by calling macrofagi and fibroblasts also serves as the inducer gene to direct fibroblast cell replication in the context of skin ulcer. Repeated application of the collagen membranes, in 8-10 days intervals, allows for the preservation of conditions that facilitate cell replication in cutaneous ulcer with reconstruction of the dermal tissue up to the total filling up of the skin ulcer to the epidermal limit. Once the connective tissue regeneration phase is completed the definitive dermal ulcer healing requires that the stage of epithelial regeneration is initiated.
Case 4 - I. G. age 80 A: Chronic skin ulcer extended to the right side of right leg dating back 1 year secondary to chronic venous and lymphatic insufficiency means loss of substance and ulcerative base about 3 mm from the skin surface. B: After 1 month of treatment with collagen therapy: reduction of the depth of the skin ulcer with ulcerative base at about 1 mm from the skin surface. C: To 3.5 months of treatment with collagen is completely filled up to the skin limit of the ulcerative base. D: Application of the collagen membrane to the periphery of the skin ulcer in order to promote epithelialisation. E - F: Removing collagen membrane previously applied through neo-epithelium below. G: Significant reduction in the extent of the lesion at 6 months of collagen therapy. H: 6.5 months. I: Complete healing 8 months after initiation of therapy.
Re-epithelialization of skin ulcers
The re-epithelialisation of skin ulcers, whether they are of recent onset or evolved in chronic skin ulcers, requires that a process of slipping and replication of epithelial cells free from trauma from is implemented the periphery towards the center. Repeated application and at 10-15 days intervals of collagen membrane placed at the outer edges of the skin ulcer enabled, in our experience, an effective and rapid re-epithelialization with a resolution of even large leg ulcers. The personal experience relates to the use of collagen membranes of varying thickness and, when aimed at initiation and preservation of the granulation process, chosen according to the extent of the loss of substance of cutaneous ulcer. The membrane in this case is totally reabsorbed from the ulcerative base and will no longer be found at the next dressing. In the phase of reepithelialization the collagen membrane used has a minimum thickness (300-400 micrometres) and acts as a protection to the sliding epithelial skin from the edges of the ulcer, will be found at the next dressing and adherent to the neo-epithelium (see description case 4) from which will be gradually removed.
Clinical Results
The clinical results with use of ultrasonic ( GENERA ULTRASONIC )treatment associated with collagen therapy in the treatment of skin ulcers of the lower extremities are by personal experience, very positive and innovative compared to conventional treatments. In particular, in addition to the benefits described above regarding the use of ultrasound related to debridement-wound cleansing and a significant reduction of the bacterial load (see article SKIN ULCERS: ULTRASONIC TREATMENT) the following has been observed:
- Effective action of collagen membranes over a primer and ready to continue with the process of granulation with tissue regeneration with total closure of skin ulcer up to the epidermal limit
- Effective action on collagen membranes reepithelialization
- High response of collagen membranes on the recovery of regenerative activity in chronic skin ulcers for years in a stabilized inflammatory state
- Action to protect the edges of the skin ulcer with reduction, locally, of inflammatory-evolutionary processes responsible for frequent extension of the lesion
- Preservation by collagen membranes of a ulcerative base cleaned with reduced apposition of fibrin
- Reducing the number of skin ulcer medications compared to conventional wound dressings, with intervals ranging from 8-10 days in the granulation phase of 10-15 days during reepithelialization
Case 5 - S. N., age 79. Skin ulcer chronic lower limb DX dating back about 5 years, the region above the medial malleolus, in patient with lower extremity PAD (bearer of femoral popliteal bypass DX) and chronic venous insufficiency from previous DVT leg DX. A: After ultrasonic treatment. B: After application of collagen membrane segments. C: 20 days after initiation of collagen therapy. Q: 52 Day E: 72 °. F day: Full healing at 134th day with collagen therapy.
Case 6 - B. Ca91 post traumatic infected ulcerative lesion in the lateral malleolar right foot dating back over 13 months. A: After ultrasonic treatment ( GENERA ULTRASONIC ) and application of collagen membrane. B: After 17 days of treatment. C: Significant reduction of ulcerative region at day 30. D: At day 42. E: Complete resolution at day 65 of treatment with collagen membrane. F: Check-up 1 month after healing of cutaneous ulcer.
EQUIPMENT:
GENERA ULTRASONIC - by Italia Medica srl - info@italiamedicasrl.com - info@italiamedicaint.com
-------------
Bibliography
1) Ultrasonic Treatment of Infected Leg Ulcers: Results Preliminary. La Rosa A. et al. 15th World Congress of Phlebology of the Union Internationale de Phlebologie - Rio de Janeiro, October 2-7, 2005 ( GENERA ULTRASONIC - by Italia Medica srl Congress ).
2) Equine Pericardium Collagen Wound Dressing in the Treatment of the Neuropathic Diabetic Foot Wound. A Pilot Study. John G. Fleischli, DPM, Terese J. Laughlin, DPM and Jeffery W. Fleischli, DPM. Journal of the American Podiatric Medical Association. Volume 99 Number 4301-305 2009
3) Knapp TR, Kaplan EN, Daniels JR. Injectable collagen for soft tissue augmentation. Plast Reconstr Surg.1977; 60:398-405.
4) Knapp TR, Luck E, Daniels JR.Behavior of solubilized collagen as a bioimplant. J Surg Res 1977; 23:96-105.
5) Greenstein G, Caton JG. Biodegradable barriers and guided tissue regeneration. Periodontol 2000. 1993; 1:36-45.
6) Schlegel AK, Mohler H, F Busch, et al. Preclinical and clinical studies of a collagen membrane (Bio-Gide). Biomaterials. 1997; 18:535-538.
Prof. Antonio La Rosa
Specialista in Chirurgia Vascolare. Chirurgia Sperimentale, Microchirurgia.
Università degli Studi di Pavia
Cell.+39 339/7994760
Tel. +39 0382/24179
www.antoniolarosa.org



Profilo del medico - Prof. Antonio La Rosa

Nome:
ANTONIO LA ROSA
Comune:
PAVIA
Telefono:
Per appuntamenti : 339 7994760 – 0382 24179
Specializzazione:
CHIRURGIA VASCOLARE
Contatti/Profili social:



